
Vertebral Ultrasound:A Window to the GreatVessels
Mindy M. Horrow, MD, FACR, FSRU
Professor of Radiology Jefferson Medical School
Director of Body Imaging
Albert Einstein Medical Center
•Goals and Objectives
•Identify the anatomy of the vertebral arterycirculation.
•Describe the spectrum of subclavian stealsyndrome.
•Describe the findings in the vertebral artery andcarotid circulation which indicate brachiocephalicdisease
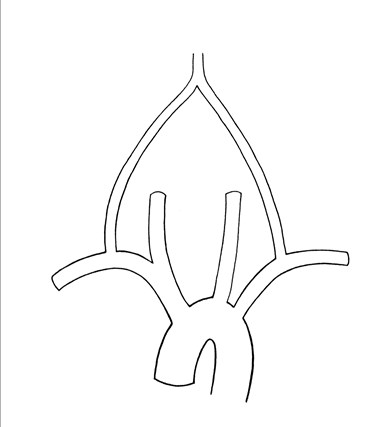
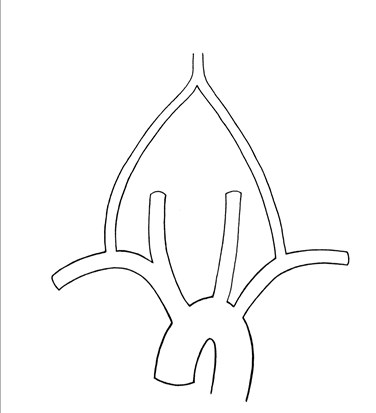
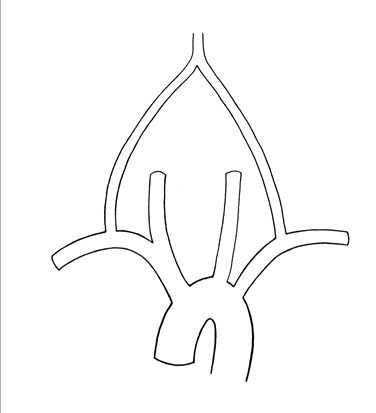
Vertebral Artery Anatomy
•First branch of subclavian artery, in 6% mayarise directly from aortic arch
•Extends from origin to entry into transverseforamen of C6, passing through to exit C1 toforamen magnum. Intracranial portion givesrise to PICA then joins with contralateral VAto form basilar artery
•Variations: hypoplastic, terminates in PICA,left VA dominant in 50 – 60%

Normal Aortic Arch (bovine variant)
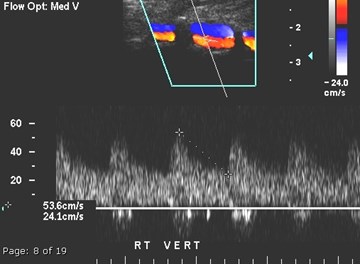
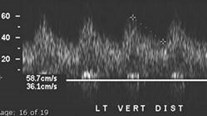
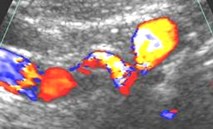
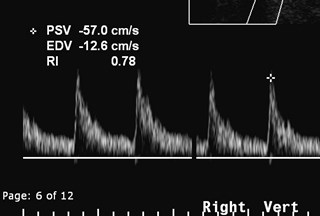
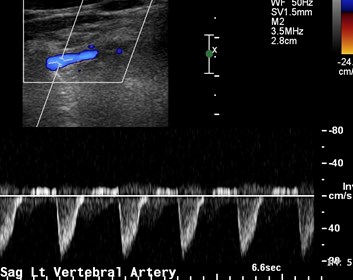
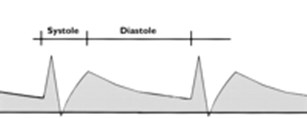
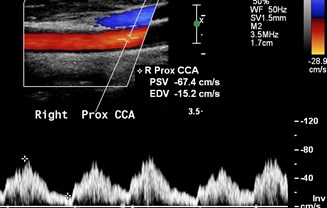
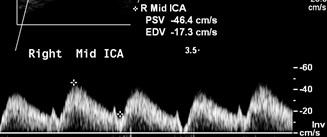
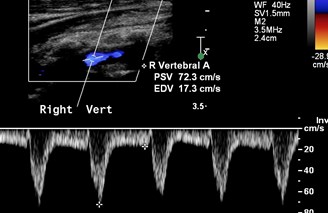
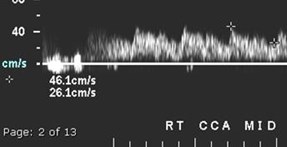
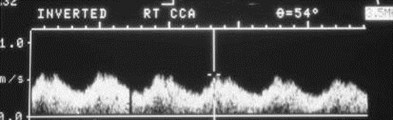
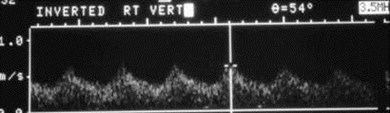
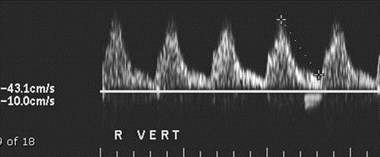
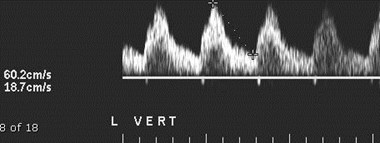
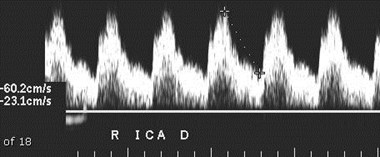
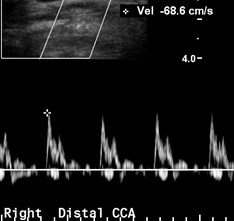
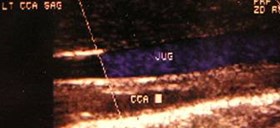
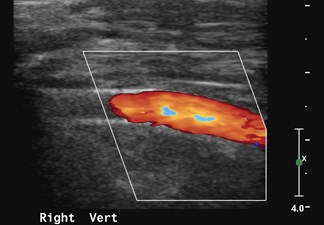
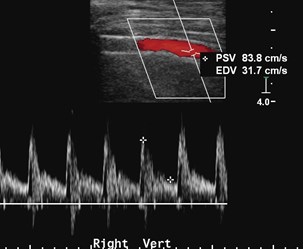
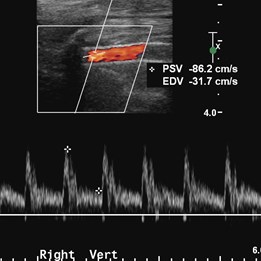
Doppler of Normal VA
Routinely imaged betweenvertebral foramina,successful imaging in 95%patients
Scanning may be extendedto proximal extra vertebralsegment and origin. Rightorigin visiualized in 92%,left in 86%
Low resistance vessel(average RI = 0.69)
Average peak systolic anddiastolic velocities are 56and 17 cm/sec
Bendick, etal. J Vasc Surg 1986; 3: 523
Trattnig, etal. Stroke 1990; 21: 1222
Colquhoun, etal. Br J Radiol 1992; 65: 1069
Tay, etal. Eur Radiol 2005; 15: 1329
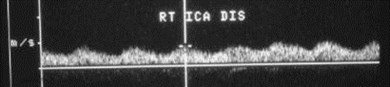
Intrinsic VA Disease
Most stenoses are ostial. May be inferred byparvus tardus waveform or imaged directly.Sen/Spe for stenoses > 70% are 71 and 99%
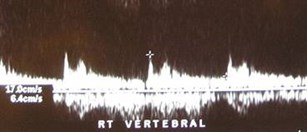
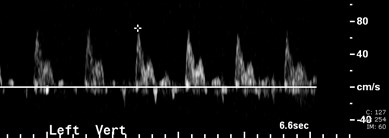
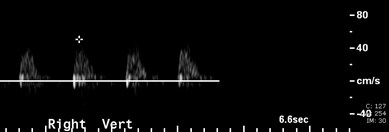
Abnormal high resistance waveform occurswith distal high grade stenosis or occlusion.May also occur with hypoplastic vessel andtermination in PICA
Dissection- US sensitive (absent flow, lowflow, absent diastolic flow) but NOT specific
Arteriovenous fistula
deBray, etal. Cerebrovasc Dis 2001; 11:335
Lu, etal. J Ultrasound Med 2000; 19:263
Yurdakul, J Ultrasound Med 2011;30:163
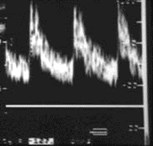
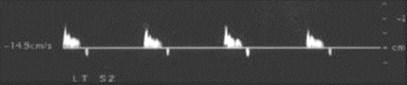
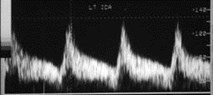
Parvus-Tardus Waveform
Tardus - pulse beat slow to rise andfall
Parvus - small pulse
Occurs
•Distal to a significant stenosis
•When vessels fill through collaterals
Kotval: J Ultrasound Med 8:435, 1989
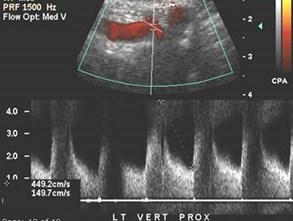

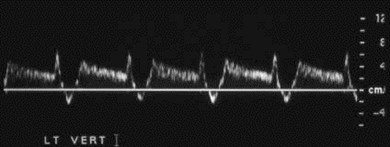
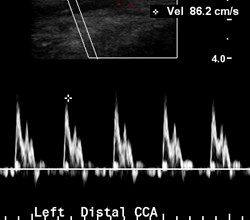
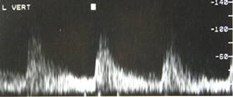
High grade stenosis at originof left vertebral artery
Use V1/V2 > 2.2, peak sys vel > 108 Cm/sec
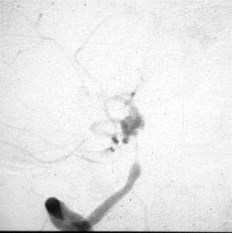
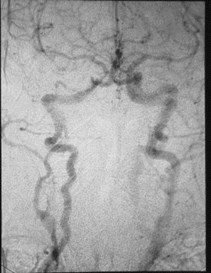
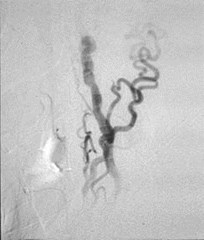
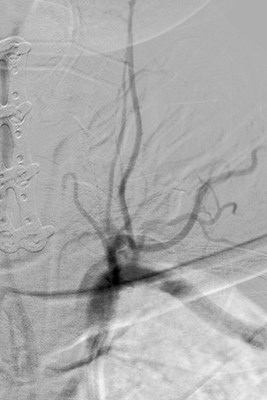
RVA INJECTION
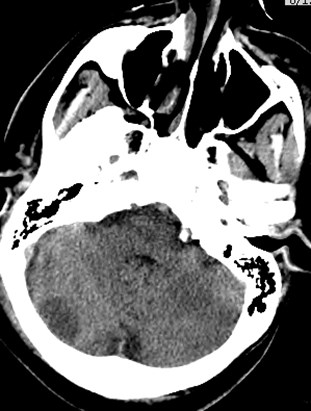
Basilar Artery Aneurysm whichbled, causing spasm of RVA
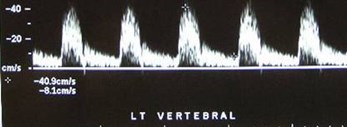
LVA
RVA
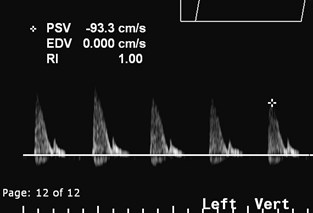

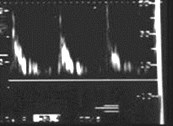
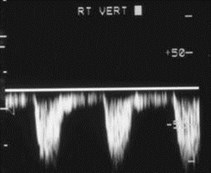
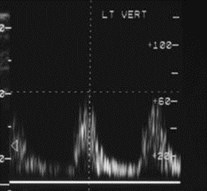
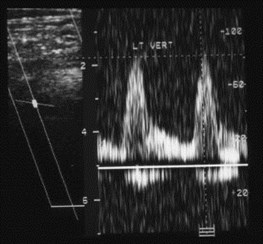
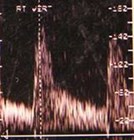
Occluded versusHypoplastic Left VertebralArtery
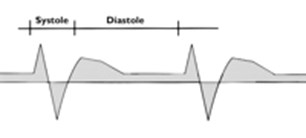
High
resistance
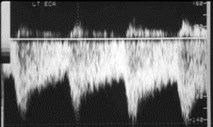
High Resistance Vertebral Artery
•Study of 79 patients with correlativeangiographic imaging
•Total 90 high resistance waveforms
•18.9 % normal
•38.9 % distal stenosis or occlusion
•35.6 % congenitally diminutive
•6.7 % other (tortuosity, FMD, basilar arteryhypoplasia)
Kim, etal. J Ultrasound Med 2010;29:1161

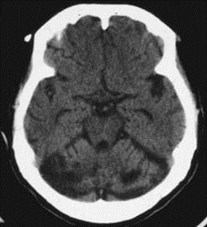
Near occlusive basilar stenosiscausing cerebellar infarcts
Subclavian Steal
•2° occlusion or near occlusion of subclavianartery proximal to origin of VA with retrogradeflow in ipsilateral VA filling via contralateral VAvia basilar artery
•First described in NEJM in 1961
•Causes: atherosclerosis most common,occasionally trauma, embolic, inflammatory,ipsilateral hemodialysis fistula, bypass grafts
•Most common clinical finding is diminishedpulse and blood pressure, also vertebrobasilarinsufficiency with arm exercise
Editorial NEJM 1961; 265: 912
Kotval, etal. J. Ultrasound Med 1989; 8:697
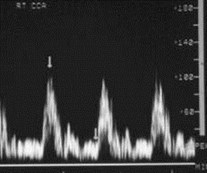
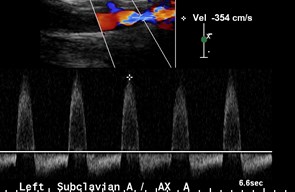
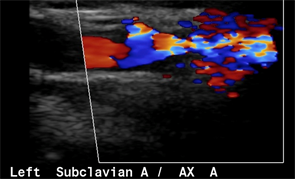
Left Subclavian Steal

Right Subclavian Steal
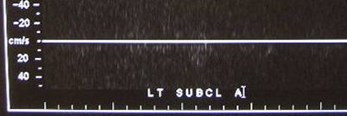
Left SubclavianOcclusion distal to LVA
Left Subclavian Stenosisdistal to LVA
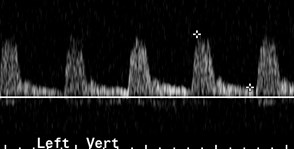
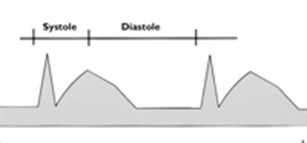
Partial Steal Physiology
Transient sharp deceleration in velocity inmid/late systole
Due to subclavian artery stenosis
Typically progresses to more severe level withinduced hyperemia
4 types: nadir of systolic notch
–> end diastole
–= end diastole
–= baseline
–Below baseline
Kliewer, etal AJR 2000; 174:815
Kotval etal J Ultrasound Med 1990; 9:207
Partial Steal Physiology
Kliewer, etal AJR 2000; 174:815
Kotval etal J Ultrasound Med 1990; 9:207
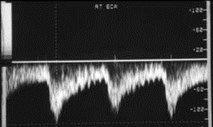
“Bunny” waveforms
Increasing subclavian stenosis
Steal Physiology
Flow in ipsilateral VA is antegrade in earlysystole. As velocity rises pressure gradientacross stenosis is great enough to behemodynamically significant.
Pressure in arm distal to stenosis becomes lowerthan pressure in vertebral system and there iseither a deceleration of antegrade flow or flowproceeds retrograde down VA into distalsubclavian a.
In diastole gradient across stenosis is low andpressure gradient disappears as distal subclaviana. reverts to normal relationship with its branchesand antegrade flow occurs.


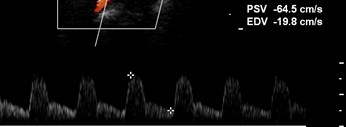
Partial Steal: LeftSubclavian Stenosis
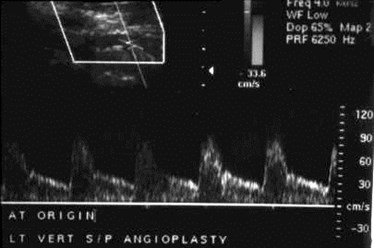
After L Subclavian artery angioplasty, LVAwaveform returns to normal
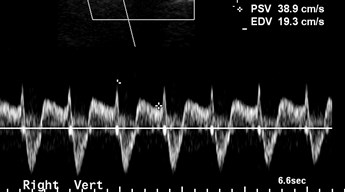
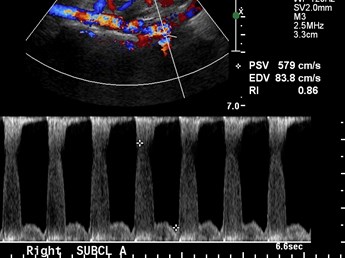
Partial Steal: RightSubclavian Stenosis
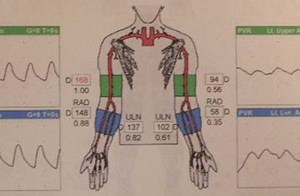
Clinical Importance of StealPhysiology in pre-CABG patients
•Small study of 13 patients showed 7 (54%) withabnormal flow in internal mammary arteryipsilateral to a VA with some degree ofreversed flow
•With completely reversed VA flow, internalmammmary artery always showed some degreeof abnormality
•In patients with in situ internal mammary graftscan result in coronary – subclavian stealsyndrome.
Ozbek etal. J Ultrasound Med 1998; 17: 147
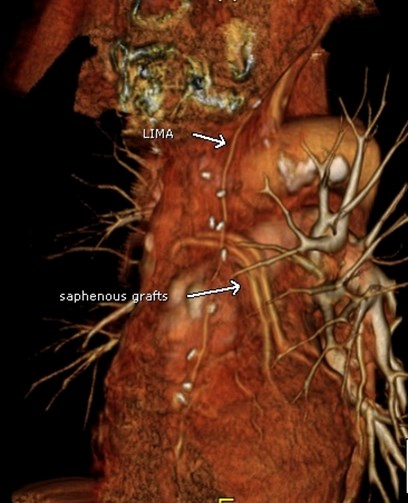

Left subclavian stenosiscauses poor LIMA inflowand resulting angina
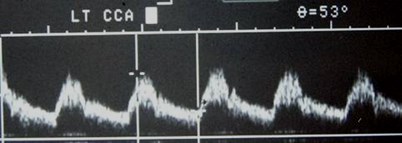
Innominate Disease
Severe stenosis or occlusion of innominatecan cause a steal physiology in RVA, but willalso effect carotid circulation.
Carotid vessels: decreased velocities,( LCCA/RCCA ), mid-systolic deceleration,parvus tardus. Variations in Dopplerabnormalities may reflect type and extent ofcollateral pathways
Grant etal. AJR 2006; 186: 394
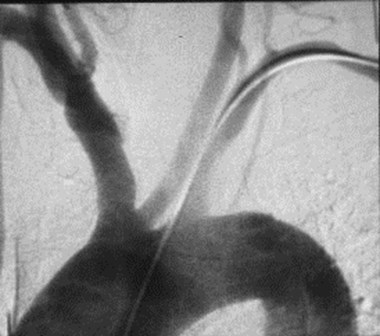
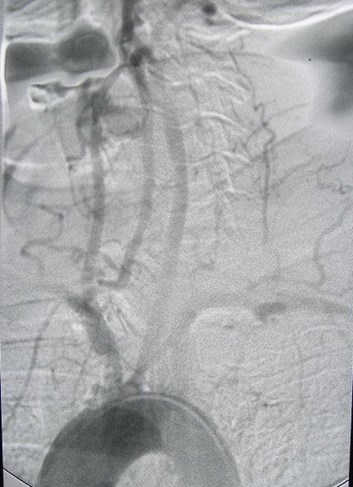
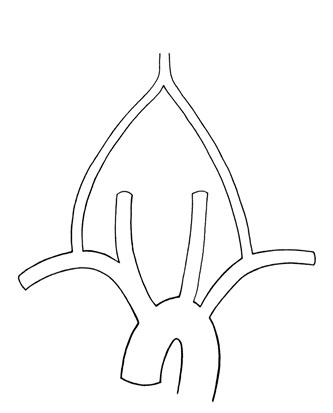
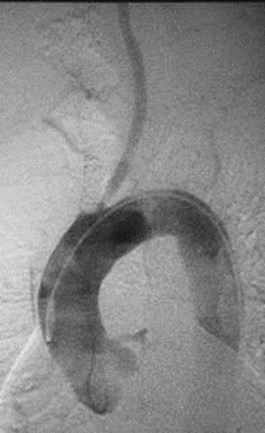
Brachiocephalic Occlusion
Brachiocephalic Occlusion



Angiographic study confirmsbrachiocephalic occlusion
Brachiocephalic Stenosis


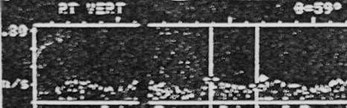
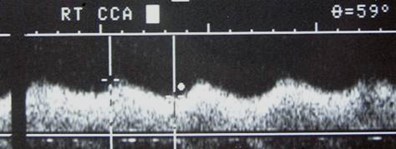
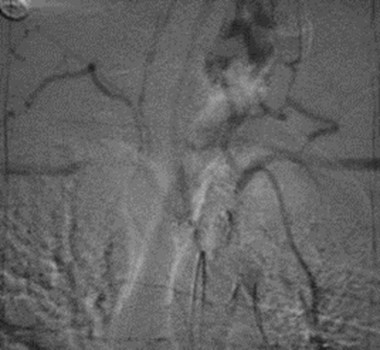
Patient with Takayasu’s Arteritis
Vertebral and subclavian arteries and rightcarotid system fill through collaterals, LCCAstenosis

Normalization of waveforms afterbypass surgery
Other Vascular Combinations
Delayed upstroke both vertebraland carotid circulations = AorticStenosis


Calcific Aortic Stenosis
Left ventricular dilatation and hypertrophy
Aortic Stenosis CausingParvus-Tardus Effect
Critical:100%
Severe:20%
Moderate/mild: 17%
Boyle et al: AJR 1996;166:197
All high resistance
Aortic Insufficiency



Occluded CCAs with increased flow invertebral arteries and collaterals toretrograde ECAs and then antegrade ICAs
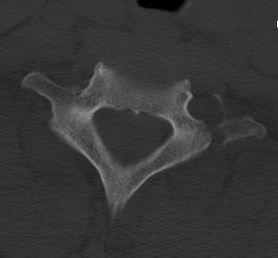

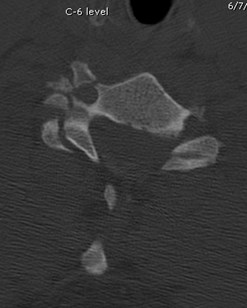
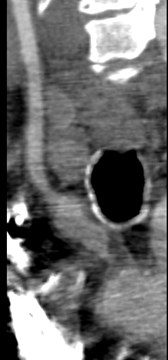
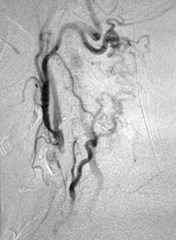
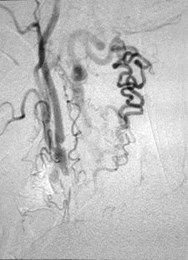
Trauma victim after MVC

CTA

Bilateral vertebral artery injuries/dissections

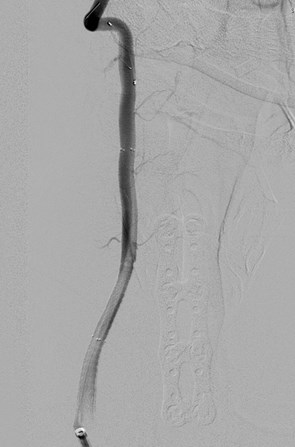

Post stent images

Post stent imaging


Kings Canyon National Park, California, August 2007
THE END
References
•Branchereau A, Magnan PE, Espinoza H, Bartoli JM: Subclavian arterystenosis: Hemodynamic aspects and surgical outcome. J CardiovascSurg 32:604-612, 1991.
•Buckenham TM, Wright IA: Ultrasound of the extracranial vertebralartery. Br J Radiol 77:15-20, 2004.
•Editorial: A new vascular syndrome – “The subclavian steal.” N Engl JMed 265:912-913, November 2, 1961.
•Grant EG, El-Saden SM, Madrazo BL, Baker JD, Kliewer MA: Innominateartery occlusive disease: Sonographic findings. AJR 186:394-400, 2006.
•Horrow MM, Stassi J: Sonography of the vertebral arteries: A window todisease of the proximal great vessels. AJR 177:53-59, 2001.
•Kliewer MA, Hertzberg BS, Kim DH, Bowie JD, Courneya DL, Carroll BA:Vertebral artery Doppler waveform changes indicating subclavian stealphysiology. AJR 174:815-819, 2000.
•Kotval PS, Babu SC, Shah PM: Doppler diagnosis of partialvertebral/subclavian steals convertible to full steals with physiologicmaneuvers. J Ultrasound Med 9:207-213, 1990.
References
Kotval PS, Shah PM, Berman H: Doppler diagnosis of subclavian stealdue to arteriovenous hemodialysis fistula in the ipsilateral arm. JUltrasound Med 8:697-700, 1989.
Lu C-J, Jeng J-S, Huang K-M, et al: Imaging in the diagnosis and follow-up evaluation of vertebral artery dissection. J Ultrasound Med19:2630270, 2000.
Ozbek SS, Parildar M: Hemodynamic disorders in internal thoracic artery:How often are they associated with subclavian steal via ipsilateralvertebral artery? J Ultrasound Med 17:147-151, 1998.
Reivich M, Holling E, Roberts B, Toole JF: Reversal of blood flow throughthe vertebral artery and its effect on cerebral circulation. N Engl J Med265:878-885, November 2, 1961.
Tay KY, U-Kin-Im JM, Trivedi RA, et al: Imaging the vertebral artery: EurRadiol 15:1329-1343, 2005.
Thomassen L, Aarli JA: Subclavian steal phenomenon. Clinical andhemodynamic aspects. Acta Neurol Scand 90:241-244, 1994.
Yip PK, Liu HM, Hwang BS, Chen RC: Subclavian steal phenomenon: Acorrelation between duplex sonographic and angiographic findings.Neuroradiology 34:279-282, 1992.